
 العربية
العربية English
EnglishLiver Diseases

What is liver?
The liver is a vital organ weighing approximately 1.2 kg in an average adult. It is located in the upper right quadrant of the abdomen.

What does liver do?
The liver is an essential organ responsible for a wide range of vital functions that keep the body healthy.
Read More
Blood from the stomach and intestines passes through the liver, where it extracts and processes nutrients. The liver produces important substances such as proteins, glucose (sugar), and fats that are necessary for growth, energy, and overall body function.
One of its key roles is producing bile, a fluid that helps digest fats and absorb fat-soluble vitamins in the intestines. The liver also synthesizes important proteins involved in blood clotting, preventing excessive bleeding when injuries occur.
Additionally, the liver acts as a natural filter by removing drugs, toxins, and harmful substances from the bloodstream, helping to cleanse and detoxify the body.
The liver also supports the immune system by identifying and fighting off harmful pathogens, protecting the body from infections.
Overall, the liver is a powerhouse organ essential for metabolism, digestion, detoxification, and immune defense.

What causes Liver disease?
Liver disease can be caused by a variety of factors, including
Read More
- Inborn metabolic disorders (genetic conditions affecting liver function)
- Anatomical abnormalities or malformations of the liver
- Bacterial and viral infections, such as hepatitis B and C viruses
- Tumors or cancer affecting the liver
- Chronic alcohol use, which can lead to liver damage and cirrhosis
- Non-alcoholic fatty liver disease (NAFLD), often related to obesity and diabetes
- Autoimmune diseases, where the body’s immune system attacks the liver
Understanding these causes helps in early diagnosis and effective treatment to prevent liver damage.

How does children liver disease differ from adults?
Liver disease in children often has different causes and characteristics compared to adults.
Read More
Many pediatric liver diseases are congenital (present at birth) or related to inborn metabolic disorders.
These conditions may become evident shortly after birth or within the first few years of life. Examples include biliary atresia, metabolic liver diseases, and genetic disorders.
In contrast, most liver diseases in adults are acquired later in life due to factors such as viral infections (like hepatitis B and C), chronic alcohol use, non-alcoholic fatty liver disease (NAFLD), autoimmune liver diseases, or tumors.
Additionally, the approach to diagnosis, treatment, and management can differ significantly between children and adults. Pediatric liver diseases often require a specialized multidisciplinary team with expertise in paediatric hepatology and surgery to address the unique needs of growing children.
Overall, early diagnosis and timely treatment are especially critical in children to prevent long-term complications and support healthy development.
Jaundice in Newborn: Act Swiftly
Jaundice that persists beyond two weeks in full-term babies and three weeks in preterm infants is considered pathological and requires further medical evaluation.
While blood group incompatibility (such as Rhesus and ABO incompatibility) is a common cause, many anatomical and functional liver disorders can also cause jaundice during the neonatal period.
These include:
- Anatomical disorders like biliary atresia and liver cysts
- Hereditary conditions such as Progressive Familial Intrahepatic Cholestasis (PFIC) and Alagille syndrome
- Metabolic disorders including galactosemia and tyrosinemia
Early diagnosis and treatment are essential to prevent serious complications and ensure the health and well-being of the newborn.
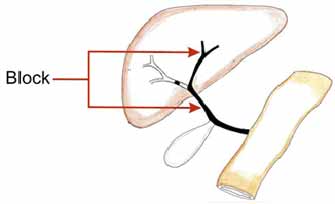
Biliary Atresia
Biliary atresia is a condition in which the bile ducts—the tubes that carry bile from the liver to the intestine—are blocked or absent. Early diagnosis is crucial to initiate timely surgical treatment.
More than half of infants who undergo the surgical procedure called portoenterostomy within the first 2 to 3 months of life successfully clear their jaundice. These children have over an 80% chance of enjoying a good quality of life and reaching adolescence without the need for a liver transplant.
Parents should watch for signs such as colorless urine and pale stools (refer to stool color charts). If there is dark urine along with suspected pale stools, consult your pediatrician immediately.
Normal
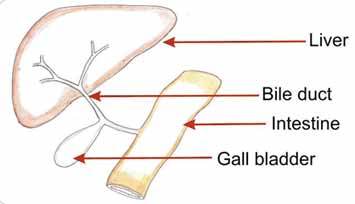
Biliary Atresia
Acute liver failure
Acute liver failure is a rapid and severe loss of liver function that can occur suddenly in a previously healthy child, leading to jaundice and impaired liver synthesis. The causes may include infections, metabolic liver disorders, autoimmune diseases, and other conditions.
In approximately 30 to 40% of cases, despite thorough investigations, the exact cause remains unknown. This condition progresses quickly and can be fatal within days if not treated promptly and appropriately.
Certain diseases, such as Wilson’s disease and autoimmune liver disorders, often do not respond adequately to medical treatment and may require liver transplantation. In contrast, some metabolic liver diseases can improve with specific dietary restrictions.
Identifying the underlying cause of liver failure is essential to determine the appropriate type of liver transplantation.
One option is an auxiliary liver transplant, where a portion of a donor liver is transplanted alongside the patient’s native liver. This approach is especially useful in cases of acute liver failure caused by infections like hepatitis A or hepatitis E. Once the acute phase resolves, the native liver can regenerate, allowing immunosuppressive medications to be discontinued. Over time, the transplanted liver gradually shrinks (atrophies), enabling the patient to live with their own liver
Alagille syndrome
Alagille syndrome is a multisystem genetic disorder characterized by a combination of distinctive features. These include a unique facial appearance—such as a triangular face, broad forehead, and pointed chin—along with cholestatic liver disease, cardiovascular abnormalities (most commonly peripheral pulmonary stenosis), eye defects (such as posterior embryotoxon), and vertebral anomalies (often butterfly vertebrae).
The severity of liver disease in Alagille syndrome can vary widely, ranging from mild symptoms like itching to severe jaundice and liver failure. While mild liver involvement can often be managed with medical treatment, severe cases may require liver transplantation.
Caroli’s disease
Caroli’s disease is a rare condition characterized by the presence of multiple cystic dilations in the bile ducts of the liver. These cysts can become infected, potentially leading to serious complications such as sepsis.
In some newborns with severe autosomal recessive polycystic kidney disease (ARPKD), extensive cystic changes in the bile ducts are observed; however, renal failure typically dominates the clinical presentation.
Ultrasound imaging of the liver is often sufficient to suggest the diagnosis of Caroli’s disease, while cholangiography provides definitive confirmation.
The prognosis largely depends on the severity of associated kidney disease and the occurrence of liver complications, such as recurrent infections, fibrosis, and portal hypertension.
Progressive familial intrahepatic cholestasis in children (PFIC)
Progressive Familial Intrahepatic Cholestasis (PFIC) is a group of inherited liver disorders that are relatively common in India. Affected infants typically present with a range of symptoms including mild to severe jaundice, low gamma-glutamyl transferase (GGT) levels, elevated serum bile acids, failure to thrive, and intense itching.
There are three recognized types of PFIC, and in some cases, the disease can also affect the intestines, leading to chronic diarrhea. Mild cases with manageable itching may respond well to medication. However, in more severe cases, a surgical procedure called biliary diversion can be performed. This surgery redirects bile flow either externally or internally, reducing the total bile acid pool in the body, which in turn decreases jaundice and itching.
For patients who progress to cirrhosis and liver failure, liver transplantation remains the only definitive treatment option. Additionally, PFIC increases the risk of liver cancer in affected children, necessitating regular and careful surveillance throughout their lives.
Non-alcoholic Fatty liver disease (NAFLD) in children
With rapid economic growth, India is facing a new health challenge among children—obesity. Fat accumulation in the liver, known as fatty liver disease, has traditionally been associated with excessive alcohol consumption in adults. However, over the past two decades, fatty liver is increasingly being detected in children, particularly in those who are obese, during routine ultrasound screenings.
While the risks of obesity and its complications are well-recognized in adults, childhood obesity is often underestimated as a serious health issue. Like adults, children with obesity can develop complications either during childhood or adolescence. The widespread availability of calorie-rich fast foods, such as fried items and pizzas, contributes significantly to the rising prevalence of fatty liver disease in India.
Currently, the prevalence of pediatric NAFLD is estimated to be around 3-10% in children with normal weight, increasing dramatically to 50-70% among obese children.
Management primarily involves lifestyle modifications, including increased physical activity and a balanced, healthy diet. Without proper intervention, NAFLD can gradually damage the liver and progress to cirrhosis, potentially necessitating liver transplantation in the future.